Treatment Chart Records
We recommend you add a treatment chart record to a patient folder after each appointment. You can type information into the record, as well as select pre-defined responses from lists, and import patient findings, appointment narratives and tooth chart data, and the next treatment sequence appointment information. In addition, authorized persons (such as the orthodontists), can verify treatment chart activity by signing the records.
Trigger a Workflow - Use the Create Treatment Chart Entry or Edit Treatment Chart Entry workflow trigger to activate a workflow whenever you create or edit a treatment chart record for a patient. (You can also trigger a workflow when a specific Treatment Chart or Treatment Plan list response is entered into a patient's treatment chart or plan. See "Treatment Chart & Plan Lists" for details.)
Evaluate Workflow Options - You can use responses from your Treatment Chart lists within a conditional element to evaluate a patient's newly-created treatment chart record. See "Workflow Conditional "If" Elements" for details.
Automate Treatment Chart Entries - Use the Create Tx. Chart Entry workflow activity to open the Treatment
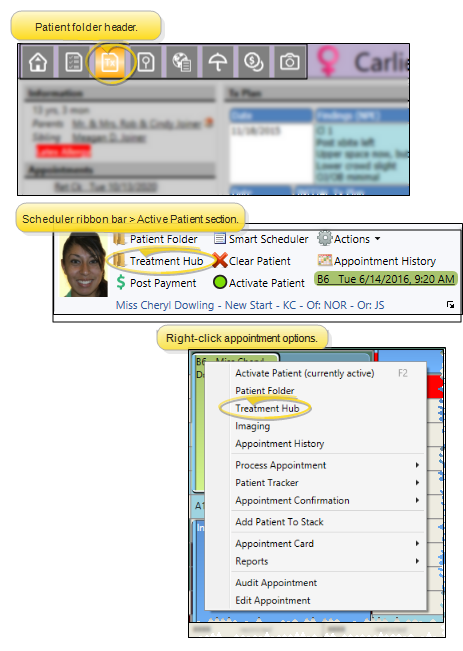
You can open the patient's Treatment Hub page by clicking the Treatment Hub icon from the patient folder header or the Scheduler ribbon bar, or by right-clicking the patient appointment in your Schedule.
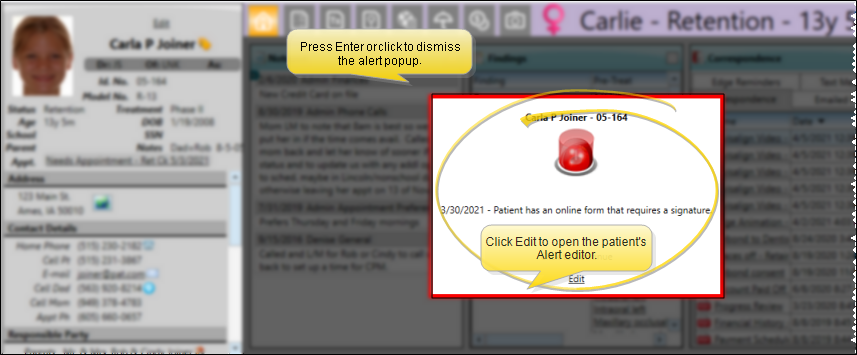
Alert Stop - If the patient has an alert trigger enabled for this feature, the Alert Stop pop-up window will appear when you initiate this feature for the patient. Review the alert information, then either press Enter on your keyboard, or click the box to continue. You can also click the Edit link to open the Alert editor for that patient.
Milestone Reminders - You may be prompted to update milestone dates when you either schedule an appointment or open the treatment chart for a patient whose Next Dental Visit and / or Next Progress Report date is either today or in the past. See "Milestone Reminders" for details.
We recommend you create a treatment chart record for each appointment you complete for a patient, and optionally integrate those records with your tooth chart, treatment sequence, and needs appointment list.
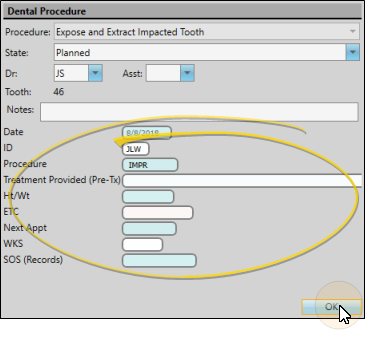
Treatment Chart Records and Dental Procedure Details - You can optionally assign a treatment chart style to a dental procedure. Then, after applying the dental procedure to a patient folder, you can edit that procedure and enter the treatment chart details. These details remain in the dental procedure record, and do not appear in as separate treatment chart records. See "About Dental Procedures" for details.
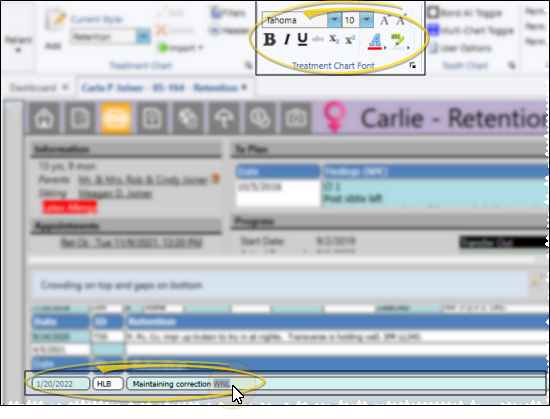
The most recently-used treatment chart style is the default for your new treatment chart record. If you would like to use a different style instead, click the Current Style drop-down in the Treatment Chart section of the Patient ribbon bar. Then choose the style to use. Your selected style will be used to create new treatment chart entries until you choose to change the style again. (See "Treatment Chart & Plan Style Editor" for details about creating your styles.)

![]() Create a Treatment Chart Record
Create a Treatment Chart Record
Records Become Permanent After 24 Hours - Once a treatment chart or plan record is 24 hours old, or after a chart record has been signed, even if that happens before 24 hours have passed, it cannot be edited or deleted. You may exit a new record you have not yet completed by pressing the Esc key on your keyboard, clicking Cancel at the bottom of the window, or exiting the patient folder before you tab out of the final column of the record. After 24 hours, or after signing a chart record, you can no longer edit the text, although you can still change the way the text looks.
Click Add in the Treatment Chart section of the Patient ribbon bar, or, right-click an existing record and select Add to create a new record with the template shown in the Current Style field. New treatment chart records are entered chronologically, with the newest entry at the bottom of the list, unless the Reverse Order option is enabled in your Treatment Chart filters. Once created, you can edit and delete the record for 24 hours. After that, the record becomes permanent.

Treatment chart and plan records can include a lot of different types of data, depending on the style you chose to create it. After entering information into a column, you can press the Tab key on your keyboard to advance to the next column, or click in the column you want to work with next. The way you enter data into a treatment chart or treatment plan column depends on the input method you select in the Column Type and List fields of the Style editor. (See "Treatment Chart & Plan Style Editor" for details about assigning column types and lists.)
Required Column Notice - Treatment chart columns that require a response when entered into the patient folder are preceded by two asterisks ( ** ), and the notice "** is a required column" appears in the window if you have at least one required column in the style. (This applies to treatment chart styles only: Treatment plan styles do not have this feature.) Once the record has been saved, the asterisks no longer appear in the column heading.
You can type text, or cut, copy, and paste You can cut, copy and paste to add and edit text and/or images to many areas of your system using standard keyboard shortcuts ( Ctrl+X , Ctrl+C , Ctrl+V , respectively). Or, you can often right-click the field or image you are working with and select the action from a menu. In many cases, Ctrl+A selects all available text or images, ready for you to cut or copy, Ctrl+Z performs an Undo of the last action, and Ctrl+Y performs a redo of the last action. text into columns that are set to either Text Only or List and Text in your Treatment Chart / Plan Style editor. In addition, while your cursor is in a Text Only or List and Text column, you can make changes to your tooth chart that will be translated into a narrative in the treatment chart column, and use the Import Findings and Import Narrative tools to add findings, appointment narratives, and treatment sequence details to the column.
Auto-Complete From Dictionary![]() - Begin typing your text in a notepad, treatment chart, or treatment plan record, then press Ctrl+Space to allow the internal Edge Cloud dictionary, as well as your personal and shared dictionaries, to suggest matching text. You can then select an entry from the list to insert into your record. (See "Edge Cloud Dictionary Editor" for details about maintaining your Edge Cloud dictionaries.)
- Begin typing your text in a notepad, treatment chart, or treatment plan record, then press Ctrl+Space to allow the internal Edge Cloud dictionary, as well as your personal and shared dictionaries, to suggest matching text. You can then select an entry from the list to insert into your record. (See "Edge Cloud Dictionary Editor" for details about maintaining your Edge Cloud dictionaries.)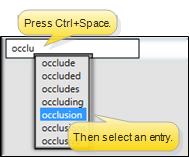
You can select responses from an assigned list for columns that are set to either List Only or List and Text in your Treatment Chart / Plan Style editor.
If you are entering data into a List Only column, you can select only one responses, and you cannot edit that response. If you are entering data into a List and Text column, you can select multiple responses from the list by pressing the space bar between responses, edit the responses, and type or copy/paste additional text as needed. In addition you can import tooth chart, findings, and appointment / treatment sequence narratives into List and Text columns, just like in Text Only columns, described above.
List responses can be set up to trigger patient rewards and workflows when entered into a treatment chart record. Also, lists may be set up to allow text search and to auto-complete.
Text Search Option![]() - When the Text Search option
is enabled for a list, you can begin typing a list response, and your cursor will jump to the response that begins with your typed text. (The matching will occur only after you have stopped typing.) If this option is disabled, your list responses will be numbered, and you can type a number to jump to the response you want.
- When the Text Search option
is enabled for a list, you can begin typing a list response, and your cursor will jump to the response that begins with your typed text. (The matching will occur only after you have stopped typing.) If this option is disabled, your list responses will be numbered, and you can type a number to jump to the response you want.
Auto Complete Option![]() - When the Auto Complete option is enabled for a list, you can press the Tab key on your keyboard to add the entirety of the currently selected response to the treatment chart / plan record. If this option is disabled, you must click the response to add the entire response text to the record.
- When the Auto Complete option is enabled for a list, you can press the Tab key on your keyboard to add the entirety of the currently selected response to the treatment chart / plan record. If this option is disabled, you must click the response to add the entire response text to the record.
You can select a response from your
Text Search / Auto Complete![]() - The Text Search and Auto Complete options are automatically enabled for Procedure List columns. This means that you can begin typing a procedure name, and your cursor will jump to the response that begins with your typed text. You can then press the Tab key to enter that response into the column.
- The Text Search and Auto Complete options are automatically enabled for Procedure List columns. This means that you can begin typing a procedure name, and your cursor will jump to the response that begins with your typed text. You can then press the Tab key to enter that response into the column.
![]() Import and Integration Options
Import and Integration Options
In addition to typing text or selecting responses from a list, you can import certain types of patient data into treatment chart records.
Import Integration Requirements - Specific Column Type and List settings are required in your Treatment Chart / Plan Styles editor before you can import data from other areas of Edge Cloud into treatment chart and treatment plan records. Be sure to review the requirements carefully if you want to use those features.
![]() Add / Deduct Patient Reward Points
Add / Deduct Patient Reward Points
Use the Patient Reward fields of your Treatment Chart List editor to add or deduct Patient Reward points for specific responses. For example, you might create an Oral Hygiene list where you award 5 points for the response "Excellent" and deduct 5 points for the response "Poor". Then assign the list to a column in one or more Treatment Chart styles. When you create a treatment chart record with that style, and a response is selected for that column, the appropriate points will be added / deducted from the patient's total.
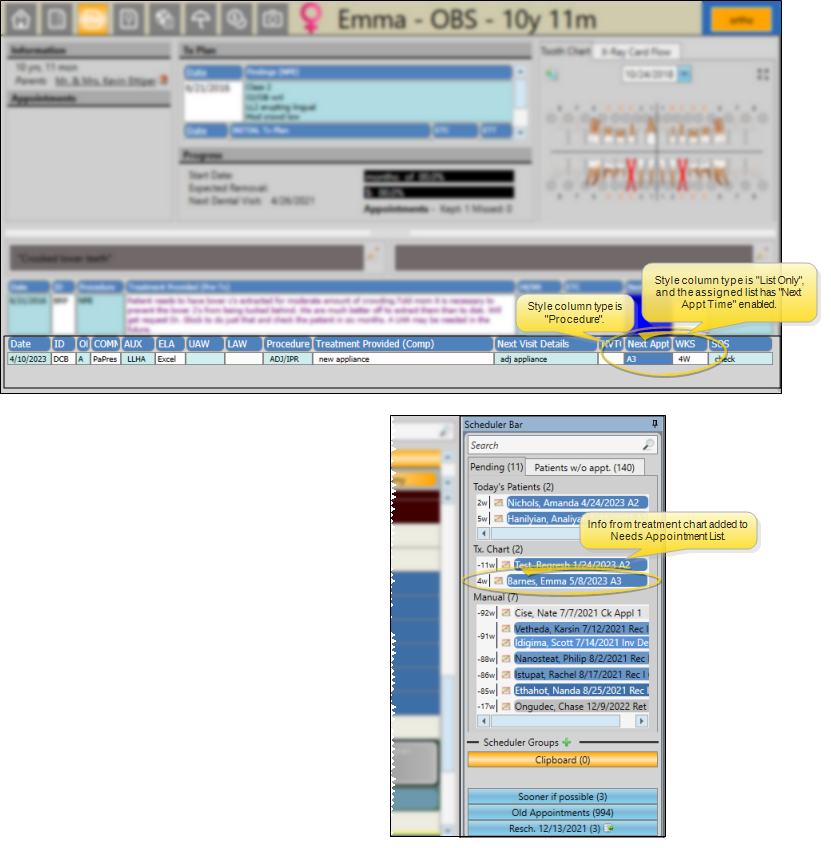
To automate adding a patient's next appointment information to your Needs Appointment list, use a treatment chart style that includes both 1) a List Only or List and Text column assigned to a list that has the Next Appt Time option enabled, and 2) a Procedure List column type. As soon as you save the treatment chart record for a patient, the Next Appt Time and Procedure that you entered into the chart will automatically transfer to your Needs Appointment List. (See "Needs Appointment List" for details.) If you select a procedure group or chain, each procedure is entered into the Needs Appointment List separately.
![]() Import Appointment and Treatment Sequence Notes
Import Appointment and Treatment Sequence Notes
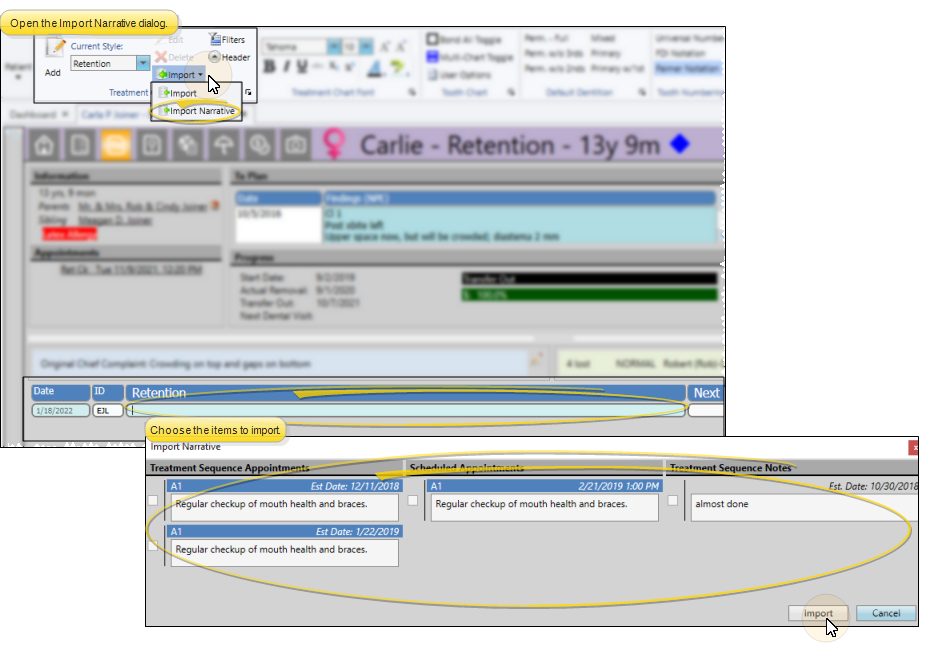
While adding data to a Text Only or List and Text treatment chart column, click the drop down button beside the  Import icon on the Treatment Chart section of the Patient ribbon bar, then select Import Narrative. (Or, press F3 on your keyboard.) You will see a window of all narratives associated with scheduled appointments, and the notes for upcoming Treatment Sequence items. Enable each narrative / note you wish to add to the treatment chart, and click Import. If you later change the narrative assigned to an appointment or treatment sequence checklist, any treatment chart records that imported the narrative will not be changed. (See "Appointment Type / Procedure Editor" for details about adding appointment narratives. See "Treatment Sequence" for detailsabout treatment sequence notes.)
Import icon on the Treatment Chart section of the Patient ribbon bar, then select Import Narrative. (Or, press F3 on your keyboard.) You will see a window of all narratives associated with scheduled appointments, and the notes for upcoming Treatment Sequence items. Enable each narrative / note you wish to add to the treatment chart, and click Import. If you later change the narrative assigned to an appointment or treatment sequence checklist, any treatment chart records that imported the narrative will not be changed. (See "Appointment Type / Procedure Editor" for details about adding appointment narratives. See "Treatment Sequence" for detailsabout treatment sequence notes.)
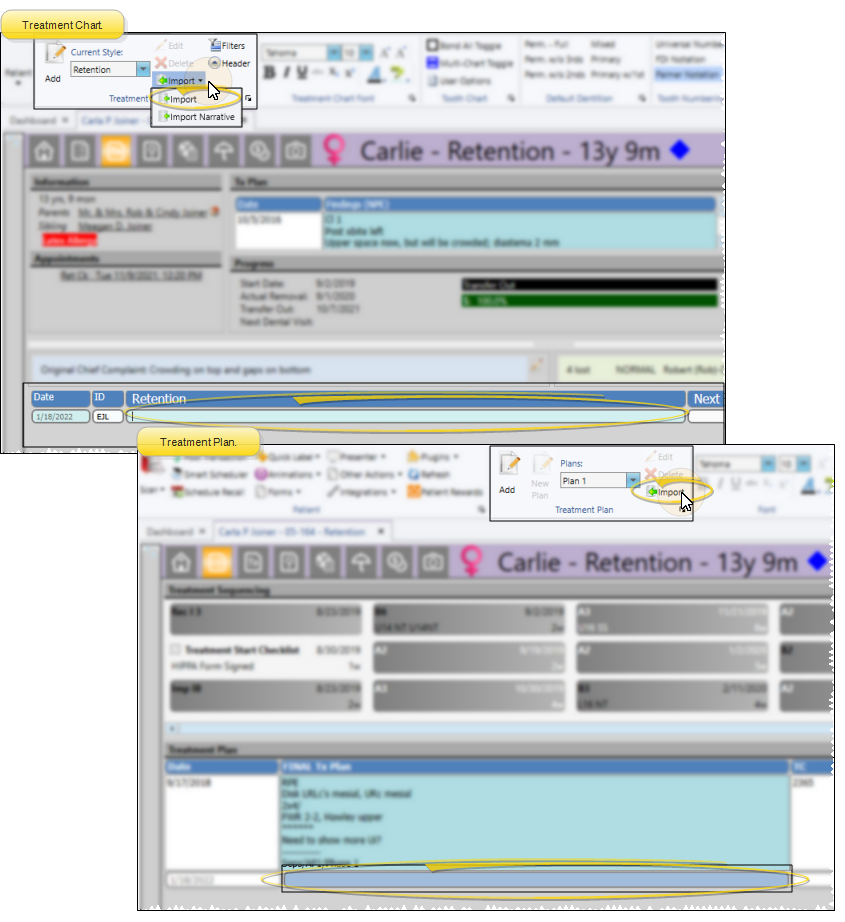
First, create a treatment chart or treatment plan record with a style that contains a column that accepts Text Only or List and Text input. With your cursor in that column, click Import from the Treatment Chart or Treatment Plan ribbon bar. Or, select Import from the Import dropdown options of the Treatment Chart ribbon, or press F2 on your keyboard. You then choose which findings to import. See "Add Findings to Treatment Plan / Chart" for details.
To include tooth chart data in your treatment chart records, first place your cursor in a Text Only or List and Text column of a new treatment chart record. Then, with that record still open, make any needed changes to the tooth chart, including adding and removing elastics. The tooth chart data will be translated into a narrative description in the active column of your treatment chart record.(You can optionally turn this feature off. See "Tooth Chart Editor" for details.)
![]() Treatment Sequence Integration
Treatment Sequence Integration
To integrate the patient's treatment sequence with their treatment chart records, use a treatment chart style that includes both 1) a List Only or List and Text column assigned to a list that has the Next Appt Time option enabled, and 2) a column with the Procedure List column type. As you create a treatment chart record for the patient, their next treatment sequence appointment information will be entered as the default for those columns. See "Treatment Sequence" for details.
Click and drag to select the text you want to work with, then use the Treatment Chart Font section of the ribbon bar to apply a new font, color or emphasis to the text. If the Rich Text option is enabled for this style column, only the selected text will be affected. Otherwise, the entire column will be affected by your formatting choices. See "Treatment Chart & Plan Style Editor" for details about enabling / disabling this style option.
Click Save in your Quick Access toolbar, or at the bottom of the window, or press your Tab key after the final column of the record to save it.
Records Become Permanent After 24 Hours - Once a treatment chart or plan record is 24 hours old, or after a chart record has been signed, even if that happens before 24 hours have passed, it cannot be edited or deleted. You may exit a new record you have not yet completed by pressing the Esc key on your keyboard, clicking Cancel at the bottom of the window, or exiting the patient folder before you tab out of the final column of the record. After 24 hours, or after signing a chart record, you can no longer edit the text, although you can still change the way the text looks.
![]() Edit and Audit Treatment Chart Records
Edit and Audit Treatment Chart Records
Records Become Permanent After 24 Hours - Once a treatment chart or plan record is 24 hours old, or after a chart record has been signed, even if that happens before 24 hours have passed, it cannot be edited or deleted. You may exit a new record you have not yet completed by pressing the Esc key on your keyboard, clicking Cancel at the bottom of the window, or exiting the patient folder before you tab out of the final column of the record. After 24 hours, or after signing a chart record, you can no longer edit the text, although you can still change the way the text looks.
You can delete only records created within the past 24 hours, and only unsigned chart records. Right-click the record you want to change, then select Delete. Or, click  Delete in the Treatment Chart / Plan section of the ribbon bar.
Delete in the Treatment Chart / Plan section of the ribbon bar.
You can edit only records created within the past 24 hours that have not been signed. Right-click the record you want to change, then select Edit. Or, click Edit in the Treatment Chart / Plan section of the Patient ribbon bar. When you finish making changes, press the Tab key on your keyboard to save them. Or, click Save in your File ribbon bar or Quick Access toolbar to save the changes.
Click and drag to select the text to work with, then you can cut, copy, and paste You can cut, copy and paste to add and edit text and/or images to many areas of your system using standard keyboard shortcuts ( Ctrl+X , Ctrl+C , Ctrl+V , respectively). Or, you can often right-click the field or image you are working with and select the action from a menu. In many cases, Ctrl+A selects all available text or images, ready for you to cut or copy, Ctrl+Z performs an Undo of the last action, and Ctrl+Y performs a redo of the last action. that text as needed.
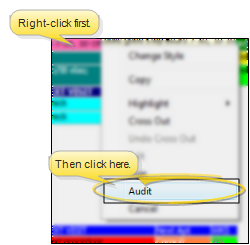
Right-click any record and select Audit to review the operator, date, and time the record was created, as well as when it was last changed.
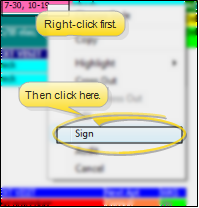
Once a treatment chart record has been saved, authorized persons, such as orthodontists, may sign it to verify the information. This feature is useful for many reasons, and especially in university settings, where entries must be double-checked for accuracy. Signed records cannot be edited, even if they are less than 24 hours old. To sign a record, right-click the entry you want to verify, and select Sign. Then enter your user name and password.
Signed records are identified by an icon ( ) at the beginning of the record
) at the beginning of the record

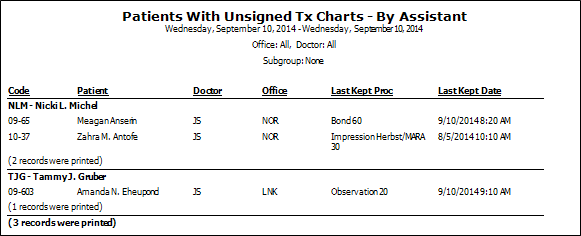
![]() Print a Report of Unsigned Treatment Charts
Print a Report of Unsigned Treatment Charts
Run the Patients with Unsigned Treatment Charts - Assistant report to review the list of the patients who have an unsigned treatment chart record that was entered within the dates you specify. The report sorts the results by assistant. See "Patients with Unsigned Treatment Charts Report" for details